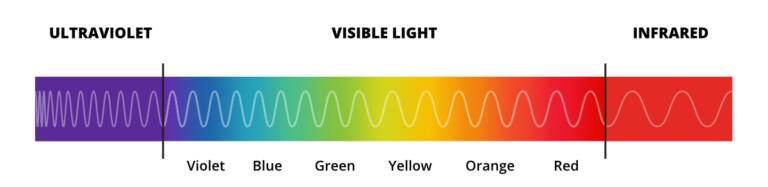
Infrared therapy (also referred to as infrared light therapy) uses mostly invisible light that sits just beyond visible red light on the electromagnetic spectrum. The wavelengths are longer than visible red light and can penetrate deeper into the body, up to a few centimetres, reaching muscles, joints and even bones.
This deeper penetration makes infrared light therapy of particular interest to sports medicine because of its potential to help alleviate deeper muscle pain, promote the repair of damaged tissues, and reduce inflammation. Supporting faster healing of injuries and enhancing post-workout recovery would make it a useful tool for athletes managing both acute and chronic injuries.
Infrared is often divided into three sub regions:
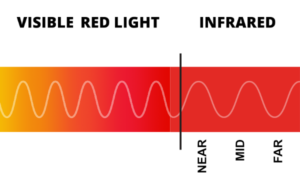
The boundaries between the three infrared wavelength regions are not widely agreed upon and can vary. Two classifications often cited in red light therapy research are ISO 20473 and CIE.
Nitric oxide (NO) plays a vital role in the human body as a vasodilator, helping to relax and widen blood vessels, which improves blood flow and oxygen delivery to tissues.
It also participates in immune response, neurotransmission and cellular signalling, influencing processes like inflammation, tissue repair and blood pressure regulation.
Light exposure stimulates mitochondria to increase the production of adenosine triphosphate (ATP), providing cells with more energy.
Cell energy is crucial for cellular functions such as repair, growth and regeneration processes.
Studies have found that in healthy cells, production of reactive oxygen species (ROS) can briefly increase, known to be beneficial for cellular signalling and repair, such as promoting wound healing and reducing inflammation.
Conversely, in oxidatively stressed cells, anti-oxidant defences are up-regulated to reduce oxidative stress.
cAMP and cGMP are cyclic nucleotides that serve as second messengers, connecting signalling pathways within cells to pathways between cells.
cAMP is typically involved in processes like metabolism, heart function, and hormone regulation.
cGMP is more closely linked to nitric oxide (NO) signalling and processes like blood vessel dilation and smooth muscle relaxation.
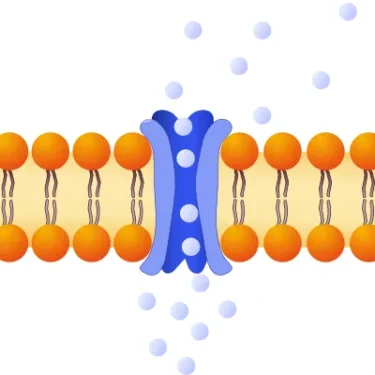
The modulation of calcium ion (Ca²⁺) levels is a significant primary effect due to calcium's central role in numerous cellular processes and signalling pathways.
Changes in intracellular calcium (calcium concentration within cells) act as secondary messengers in various signalling pathways, including those involved in muscle contraction, inflammation, repair and gene expression.
In studies inflammation reduction is one of the most reproduced physiological effects.
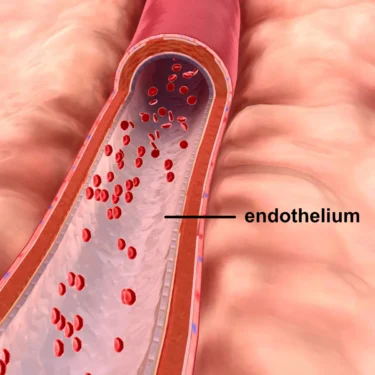
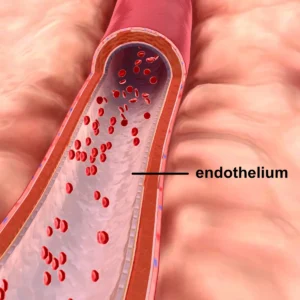
Nitric oxide (NO) inhibits the activation and adhesion of immune cells, such as neutrophils and macrophages, to the endothelium, reducing their infiltration into inflamed tissues.
It also downregulates the production of pro-inflammatory cytokines like TNF-α and IL-6 while promoting the expression of anti-inflammatory cytokines such as IL-10.

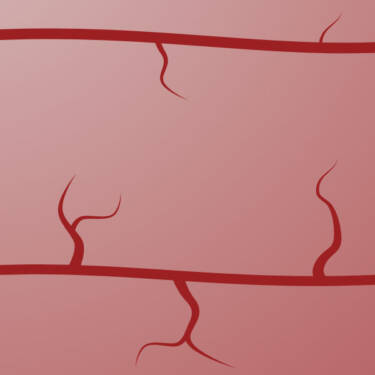
The increased nitric oxide (NO) promotes vasodilation, the process by which blood vessels widen or relax, allowing more blood to flow through them.
NO relaxes the smooth muscle cells in the walls of blood vessels, causing them to widen and increase their diameter.

Vasodilation reduces vascular resistance and improves blood flow, allowing more oxygen and nutrients to reach tissues, and facilitates the removal of metabolic waste.
Additionally, anti-inflammatory signalling reduces pro-inflammatory molecules such as cytokines and reactive oxygen species (ROS), which can cause vascular stiffness and constriction.
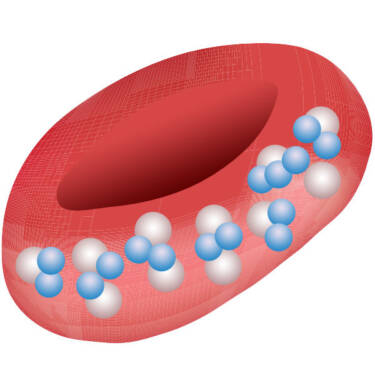
Enhanced blood flow from vasolidation increases the supply of oxygen-rich blood to tissues, supporting cellular metabolism and recovery.
Additionally, enhanced mitochondrial activity promotes more efficient oxygen utilisation, indirectly supporting oxygen availability within cells.
Research has shown moderate increases of reactive oxygen species (ROS) and oxidative stress in normal cells, beneficial for cellular signalling and repair, such as promoting wound healing and reducing inflammation.
Conversely, in oxidatively stressed cells, anti-oxidant defences are up-regulated to reduce ROS and oxidative stress.
The activation of mitochondria enhances cellular metabolism and stimulates the expression of proteins like TGF-β1, which play a critical role in regulating endothelial cell proliferation, migration and the formation of new blood vessels (angiogenesis).
This has been identified as one of the key mechanistic responses that result in benefits to wound healing, tissue repair and regeneration.

It's known that infrared light can promote the expression of growth factor proteins such as TGF-β1. They stimulate fibroblasts to produce collagen, which is essential for rebuilding the extracellular matrix and providing structural integrity to damaged tissue.
TGF-β1 also controls inflammation and promotes angiogenesis (the formation of new blood vessels), crucial for effective tissue repair and regeneration.
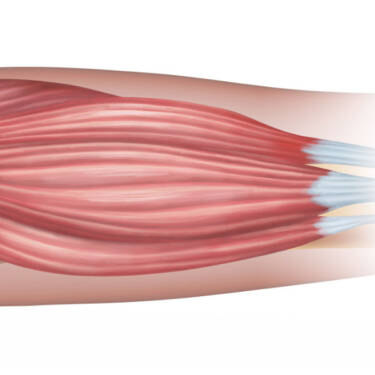
Several of the therapeutic processes already described - reduced inflammation, increased blood flow and oxygen levels, metabolic waste removal, and modulation of oxidative stress - work together to induce soft tissue relaxation.
In the muscle tissues, this has been shown to help in reducing muscle stiffness and promote proper muscle function.

Alleviating pain occurs through peripheral and central effects.
Peripheral effects involve reducing inflammation and modulating pain signals at the site of injury - modulating pro and anti inflammatory cytokines, stimulating immune cells, and reducing the expression of receptors associated with pain transmission.
Central effects involve lowering levels of inflammatory cytokines and receptors involved in transmitting pain signals within the nervous system.
The endothelium is a single layer of cells that lines the interior surface of blood vessels and lymphatic vessels throughout the body, playing a crucial role in regulating blood flow, clotting, and the exchange of substances between the bloodstream and surrounding tissues.
The heat produced by MIR and FIR can cause vasodilation, the process by which blood vessels widen or relax, improving circulation.
This increased blood flow can help deliver more oxygen and nutrients to tissues, whilst aiding in the removal of metabolic waste.

The heat generated by MIR and FIR can help reduce inflammation by increasing blood flow and promoting the relaxation of tissues.
This is more of a secondary effect of the heat rather than the direct cellular mechanism found in PBM.

The deep heating effect of FIR can help relieve muscle pain and joint stiffness, making it useful for various musculoskeletal conditions.
This pain relief may be due to both the direct effects of heat and the increased circulation.

Heat from MIR and FIR can induce thermoregulation, triggering sweating and assisting the body in maintaining an optimal internal temperature.
This process can help remove toxins from the body.

Mid-infrared light is primarily absorbed by water molecules in the skin, generating mild heat in the superficial layers of tissue.
With far-infrared, the absorption by water in tissues is greater. The resulting heat generated at the skin's surface is then transferred to deeper tissues through the body's natural heat conduction mechanisms, primarily via blood circulation.
FIR is often noted for its ability to induce sweating at lower ambient temperatures compared to MIR.
FIR also produces biological effects at lower ambient temperatures than traditional heat therapy, allowing for longer application times and potentially more widespread effects.
Some studies suggest FIR therapy may have beneficial effects on blood pressure and heart function.
FIR induces a more vigorous sweat at a lower temperature than traditional heat therapy. As the body works to cool itself (thermoregulation), the heart rate and cardiac output increases with a cardiovascular demand similar to that of a moderate pace walk.